I remain grateful to the authors of the BMJ article for highlighting this “pain in the backside” that has been troubling me for the past few years. They rightly mention that Stage III CKD may not be all that it sounds like. It was music to my ears.
The changeover from Acute renal failure to AKI and Chronic renal failure to CKD happened slowly, but felt like an overnight attempt for many of the older generation accustomed to the older terminology. Change for change's sake was not the concern; instead, change that increased confusion with diversion of resources to a bogeyman blown out of proportion, was the main reason for annoyance for many.
The new generation of practitioners who adore protocols, pathways and guidelines, love one another thing. Scores. Scoring everything makes life much easier. Whether it is a decision on who can go home to who will die in 24 hours. Live and die by the score. How then could the ease of five different stages of diagnosis based on another easy-to-do measurement not tickle the fancy of the vast majority? Without doubt it did. Subdivisions of some of the stages with added alphabets gave diagnoses a more authentic feeling. Discharge summaries never looked so good. Clinic letters carried more weight with those alphabets on. CKDIIIbp. Impressive. Communication at its best. LOL, TTYL. CKDIV. It all fitted in.
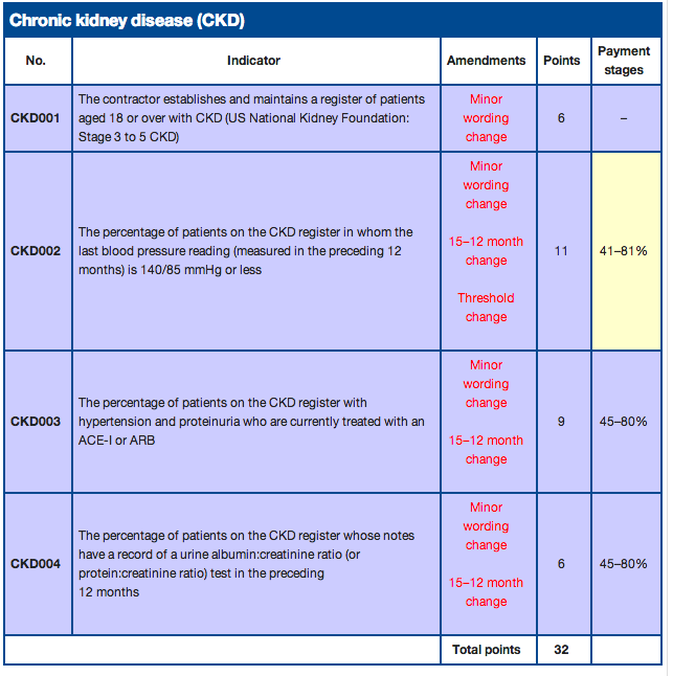
Various organisations, full to the brim with think-tanks, have been sitting around tables on their aching bottoms, trying to decide whether 2 is same as 3, or is 3 as bad as 4. Was 3a worse than 3b or was it 3ap that was the troublemaker? By this stage, only a select few maintained interest in the nitty gritty of it. The rest of the world of generalists waited eagerly for the final decisions to be made so that they could continue with their work; work that mostly involved hunting for those individuals with the appropriate stages, so that they could be called by their true name, complete with suffixes! Why was that important? Because it was important to get the diagnosis right. Why was it important to get the diagnosis right? Because it was a disease. Which meant, that there would be performance indicators on how we, the good people in the NHS, manage the disease. If the complex scoring did not appeal to your senses, the QOF monies probably would. (see picture below)
But those skeptics out there ( a dwindling resource, just like the witches of bygone era) despite fear of the stake, started speaking out in their own small realms about how the early stages of chronic kidney changes (CKC?) was a measurement sold as a diagnosis. Just like cholesterol perhaps. Just like IFG and IGT perhaps. Just like an osteopenic DEXA scan report. Just like a lowish testosterone in the ageing gentleman. But these days who is to complain? After all, we live in a world where obesity is a disease!
The crusaders for the new definitions chanted that unless something was labelled as a disease, no one would take interest in screening for it, so as to identify it early, so that a whole host of life-extending medications could be given out to outwardly healthy looking, not-a-care-in-the-world individuals who were enjoying their life just about till then. 94 year old Martha thought she was healthy. Little did she know that her risk for death in the next 10 years was close to 99%. But now, with the help of the new CKDIIIap diagnosis, she will be able to understand the relative risk for all-cause and cardiovascular mortality and take measures to reduce her risk for death in the next decade. She would also have understood that her neighbour Susan, who had CKDIII a (but no p) would be more blessed and live till 104 easily. Even if Martha didn’t understand it and didn't give two hoots about it, her new SHO-turned-GP who was au fait with CKD staging would care. He would embark on urgent screening for microalbuminuria, dipstick for haematuria, culture urine to rule out any infections, check for anaemia and hyperparathyroidism, and arrange an ultrasound scan of the kidneys at the local hospital (which is now 60 miles away because the local one was no good at identifying CKDIII and had to be closed). He wouldn’t stop there though. He has been told by the guideline that anything that moves with CKD diagnosis should get antihypertensive treatment to normalise blood pressure to pre-pubertal levels. Full dose ACE inhibitor, Aspirin and Statin to be collected from Lloyds pharmacy please. News of Granny breaking her leg due to a fall because of low blood pressure and admitted to hospital where she bled to death from a peptic ulcer was merely collateral damage. For the greater good. So that many other nonagenarian lives may be saved. After all, that is what doctors do. They save lives. Prevent death. Totally.
Whenever kids get killed in the US by a psycho with a gun, the gun lobby comes out to say that it is the man who pulls the trigger that kills and not the gun. The gun was a harmless device apparently till the perpetrator decide to convert it into a deadly weapon by activating it. Whether it is diagnosing ACS using a troponin rise, or CKD using eGFR values, or DVT using D dimer, ultimately it is a weapon that we offered to a psycho. The weapon was not a wrong thing totally, albeit a weapon but the real question is, do you want to give it to the psychos? Are responsible individuals interpreting the test and titrating investigations and treatment in an individualised manner? Who is to police, once the weapons have been dished out? Interestingly, guidelines state that CKDIII does not require referral to the specialist!!. So the psychos are now alone with a gun and told to seek help only if their urges get out of hand. I am not saying that all the new generation of doctors are psychos, just some of them
So, what is the solution to all this confusion? Brave the jeers of "politically incorrect" and "double standards" and state that after 80 years of age, eGFRs may fall physiologically just like memory and muscle mass rather than pathologically in every instance, and adjust the nomograms to reflect that? Do we dare say that statement for fear of ageism? Do we bring back geriatrics as a speciality so that only a select few may think of the elderly differently and interpret eGFR in the right context and abide by primum non nocere? Or do we do the decent thing and select students who have the head screwed on right into medical schools and then try to teach them how to individualise care in every instance, how to use guidelines as a floodlight and not as a flashlight, and above all help them develop into true doctors who are happy to stand up and say, "not everybody requires treatment for everything measured"??
The changeover from Acute renal failure to AKI and Chronic renal failure to CKD happened slowly, but felt like an overnight attempt for many of the older generation accustomed to the older terminology. Change for change's sake was not the concern; instead, change that increased confusion with diversion of resources to a bogeyman blown out of proportion, was the main reason for annoyance for many.
The new generation of practitioners who adore protocols, pathways and guidelines, love one another thing. Scores. Scoring everything makes life much easier. Whether it is a decision on who can go home to who will die in 24 hours. Live and die by the score. How then could the ease of five different stages of diagnosis based on another easy-to-do measurement not tickle the fancy of the vast majority? Without doubt it did. Subdivisions of some of the stages with added alphabets gave diagnoses a more authentic feeling. Discharge summaries never looked so good. Clinic letters carried more weight with those alphabets on. CKDIIIbp. Impressive. Communication at its best. LOL, TTYL. CKDIV. It all fitted in.
Various organisations, full to the brim with think-tanks, have been sitting around tables on their aching bottoms, trying to decide whether 2 is same as 3, or is 3 as bad as 4. Was 3a worse than 3b or was it 3ap that was the troublemaker? By this stage, only a select few maintained interest in the nitty gritty of it. The rest of the world of generalists waited eagerly for the final decisions to be made so that they could continue with their work; work that mostly involved hunting for those individuals with the appropriate stages, so that they could be called by their true name, complete with suffixes! Why was that important? Because it was important to get the diagnosis right. Why was it important to get the diagnosis right? Because it was a disease. Which meant, that there would be performance indicators on how we, the good people in the NHS, manage the disease. If the complex scoring did not appeal to your senses, the QOF monies probably would. (see picture below)
But those skeptics out there ( a dwindling resource, just like the witches of bygone era) despite fear of the stake, started speaking out in their own small realms about how the early stages of chronic kidney changes (CKC?) was a measurement sold as a diagnosis. Just like cholesterol perhaps. Just like IFG and IGT perhaps. Just like an osteopenic DEXA scan report. Just like a lowish testosterone in the ageing gentleman. But these days who is to complain? After all, we live in a world where obesity is a disease!
The crusaders for the new definitions chanted that unless something was labelled as a disease, no one would take interest in screening for it, so as to identify it early, so that a whole host of life-extending medications could be given out to outwardly healthy looking, not-a-care-in-the-world individuals who were enjoying their life just about till then. 94 year old Martha thought she was healthy. Little did she know that her risk for death in the next 10 years was close to 99%. But now, with the help of the new CKDIIIap diagnosis, she will be able to understand the relative risk for all-cause and cardiovascular mortality and take measures to reduce her risk for death in the next decade. She would also have understood that her neighbour Susan, who had CKDIII a (but no p) would be more blessed and live till 104 easily. Even if Martha didn’t understand it and didn't give two hoots about it, her new SHO-turned-GP who was au fait with CKD staging would care. He would embark on urgent screening for microalbuminuria, dipstick for haematuria, culture urine to rule out any infections, check for anaemia and hyperparathyroidism, and arrange an ultrasound scan of the kidneys at the local hospital (which is now 60 miles away because the local one was no good at identifying CKDIII and had to be closed). He wouldn’t stop there though. He has been told by the guideline that anything that moves with CKD diagnosis should get antihypertensive treatment to normalise blood pressure to pre-pubertal levels. Full dose ACE inhibitor, Aspirin and Statin to be collected from Lloyds pharmacy please. News of Granny breaking her leg due to a fall because of low blood pressure and admitted to hospital where she bled to death from a peptic ulcer was merely collateral damage. For the greater good. So that many other nonagenarian lives may be saved. After all, that is what doctors do. They save lives. Prevent death. Totally.
Whenever kids get killed in the US by a psycho with a gun, the gun lobby comes out to say that it is the man who pulls the trigger that kills and not the gun. The gun was a harmless device apparently till the perpetrator decide to convert it into a deadly weapon by activating it. Whether it is diagnosing ACS using a troponin rise, or CKD using eGFR values, or DVT using D dimer, ultimately it is a weapon that we offered to a psycho. The weapon was not a wrong thing totally, albeit a weapon but the real question is, do you want to give it to the psychos? Are responsible individuals interpreting the test and titrating investigations and treatment in an individualised manner? Who is to police, once the weapons have been dished out? Interestingly, guidelines state that CKDIII does not require referral to the specialist!!. So the psychos are now alone with a gun and told to seek help only if their urges get out of hand. I am not saying that all the new generation of doctors are psychos, just some of them
So, what is the solution to all this confusion? Brave the jeers of "politically incorrect" and "double standards" and state that after 80 years of age, eGFRs may fall physiologically just like memory and muscle mass rather than pathologically in every instance, and adjust the nomograms to reflect that? Do we dare say that statement for fear of ageism? Do we bring back geriatrics as a speciality so that only a select few may think of the elderly differently and interpret eGFR in the right context and abide by primum non nocere? Or do we do the decent thing and select students who have the head screwed on right into medical schools and then try to teach them how to individualise care in every instance, how to use guidelines as a floodlight and not as a flashlight, and above all help them develop into true doctors who are happy to stand up and say, "not everybody requires treatment for everything measured"??
 RSS Feed
RSS Feed